Diplopia, colloquially referred to as “double vision,” is a challenging chief complaint in the emergency department. The etiologies are vast. Acute life-threatening causes include stroke, aneurysm, or increased intracranial pressure. Less urgent chronic causes can include decompensated phoria (ie, misalignment of the eyes) or slowly evolving microvascular disease. Life- and organ-threatening causes should be the top concern in the emergency department, and emergency physicians must be prepared to identify any related conditions.1
Clinicians must first determine whether the patient has monocular or binocular diplopia. Monocular diplopia is confirmed when covering the opposite eye fails to resolve the diplopia. This strongly suggests etiologies that are nonemergent but should be referred for outpatient ophthalmologic evaluation. (Note: Some exceptions such as multiple sclerosis, seizures, or various forms of encephalopathy will be apparent by other aspects of the patient’s presentation.)2 The remainder of this article discusses binocular diplopia (henceforth referred to as diplopia), which occurs due to misalignment of the visual axes.
Neuroanatomy
A brief review of the neuroanatomy of eye movement is helpful to recognize patterns of extraocular muscle weakness, identify cranial nerve (CN) palsies, and localize structural lesions. Proper eye alignment and movement depend on extraocular muscles innervated by CNs III, IV, and VI (see Table 1 and Figure 1). These CNs originate in the midbrain and pons, course through the subarachnoid space near important structures such as the posterior communicating artery, travel through the cavernous sinus, enter the orbit through the superior orbital fissure, and finally innervate their target extraocular muscle(s) at the neuromuscular junction. Pathology at any of these locations may cause diplopia.
A complete CN III palsy impairs eye supraduction (vertical upward glance), infraduction (vertical downward glance), and adduction. This causes the eye to rest in a “down and out” position. An incomplete CN III palsy will present with varying degrees of weakness in each of the affected extraocular muscles. Additionally, CN III contains motor fibers that control the levator muscle of the eyelid and parasympathetic fibers located on the periphery of the nerve trunk that control pupil constriction. Compressive lesions such as aneurysms will usually (but not always) result in pupil dilation with some degree of oculomotor dysfunction and/or ptosis.
Clik here to view.
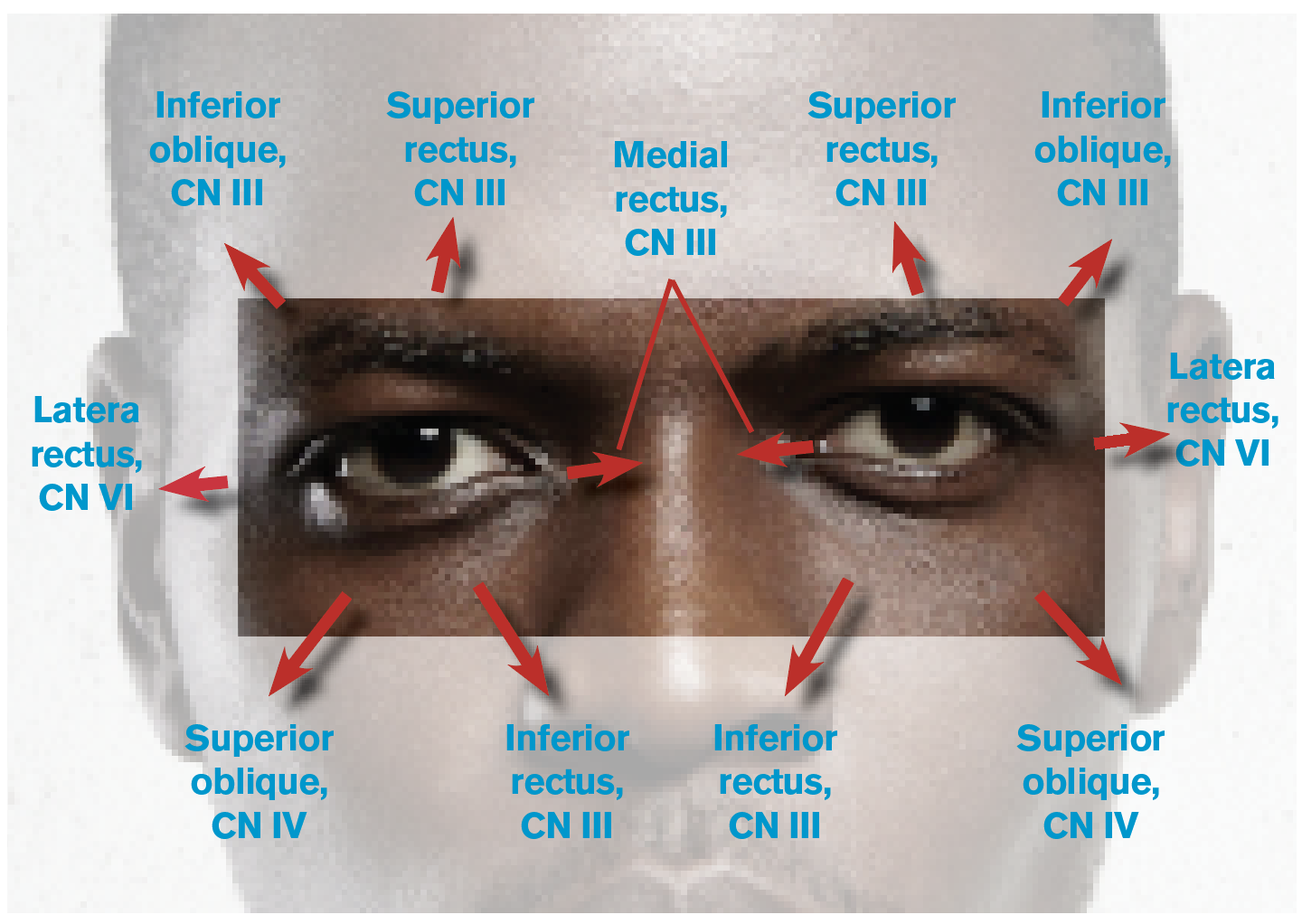
Figure 1: Eye Movements and the Related Cranial Nerves (CNs) and Extraocular Muscles
CN IV palsy causes upward deviation and rotational misalignment; however, this can be difficult to identify due to the compensatory effect of other intact extraocular muscles. To diagnose an isolated unilateral CN IV palsy, the examiner should assess whether the upward deviation in the affected eye worsens with gaze toward the contralateral side and with the head tilted toward the ipsilateral side. If the exam is not consistent with these findings, one should consider alternative diagnoses.
Clik here to view.

(click for larger image) Table 1: Eye Movements and Corresponding Extraocular Muscles
CN VI palsy is easier to identify: Patients present with medial deviation most apparent when looking toward the affected side. It is important to note that CN VI is particularly susceptible to traction caused by structural lesions or elevated intracranial pressure, a cause particularly suggested by the presence of a bilateral CN VI palsy.
Considerations for the History and Exam
Emergency physicians must first determine whether the patient has isolated diplopia or diplopia with additional neurological deficits suggestive of a posterior circulation stroke. Patients presenting with acute-onset diplopia in combination with altered mental status, bulbar weakness (such as difficulty with speech and swallow, facial muscle use, or emotional volatility), vertigo, or “crossed” brain stem signs (ie, ipsilateral CN deficits with contralateral limb weakness or sensory loss) should be considered to have a brain stem stroke until proven otherwise. The clinician should activate institutional stroke protocols, obtain neurology consultation, and obtain neuroimaging (including an MRI after a screening CT has been obtained) as soon as possible.
After a posterior circulation stroke has been excluded, clinicians should gather a thorough history as well as perform comprehensive neurological and eye exams. It is important to determine the orientation of the diplopia (horizontal, vertical, or oblique) and whether the diplopia worsens in a particular direction of gaze. This will help to identify the extraocular muscles and/or cranial nerves affected. The onset and timing of diplopia can also aid in diagnosis. Intermittent diplopia that worsens with fatigue and later in the day is suggestive of myasthenia gravis. Slowly progressive diplopia may suggest a compressive cause (eg, inflammatory, infectious, neoplastic, or vascular lesions), whereas intermittent diplopia may be due either to a decompensating phoria or myasthenia gravis.
Pain associated with diplopia can be seen in a variety of conditions. Pain localizing to the eye or retrobulbar region—particularly pain that worsens with eye movement—suggests pathology of the cavernous sinus, orbit, and/or extraocular muscles such as Tolosa-Hunt syndrome (a condition believed to be caused by inflammation of either the cavernous sinus or the superior orbital fissure), thyroid eye disease, infection, or malignancy. Microvascular ischemia and optic neuritis can also cause pain in a similar distribution. Diplopia accompanied by headache can occur in giant cell arteritis, cavernous sinus thrombosis, pituitary apoplexy (bleeding), intracranial aneurysm, cervical artery dissection, and a variety of other conditions. As always, severe or thunderclap headache suggests aneurysmal subarachnoid hemorrhage, which may be associated with aneurysmal compression of cranial nerves, most commonly CN III.
However, painless diplopia does not exclude serious neurological conditions, such as aneurysms, as pain is an unreliable finding in many conditions.3 Rarely, giant cell arteritis may present with diplopia in the absence of headache or other systemic symptoms. Accordingly, all patients over the age of 55 with double vision should undergo laboratory screening with erythrocyte sedimentation rate, C-reactive protein, and complete blood count.4,5
Internuclear ophthalmoplegia (INO) is an ocular motility disorder of horizontal conjugate gaze that is important to recognize. INO occurs due to a lesion in the medial longitudinal fasciculus of the brain stem, most commonly from multiple sclerosis or ischemic stroke. When a patient with INO attempts to look away from the affected side, there is impaired ipsilateral eye adduction and nystagmus of the contralateral eye on abduction. This may occur with conjugate gaze toward one or both sides. Convergence is usually preserved.
Diplopia occurring after head trauma may be due to decompensated phoria, CN palsies due to stretch injury or skull fracture, intracranial hemorrhage, direct extraocular muscle damage, extraocular muscle entrapment due to orbital fracture, orbital compartment syndrome resulting from a retrobulbar hematoma, or carotid-cavernous fistula. A noncontrast head CT should be the first neuroimaging obtained in trauma patients presenting with diplopia.
The patient’s past medical history can also suggest potential causes for diplopia. Patients with a history of malignancy should be suspected to have diplopia due to perineural spread or lesions in the orbit or brain. Patients suffering from chronic alcoholism may develop Wernicke encephalopathy characterized by altered mental status, gait ataxia, and oculomotor dysfunction. A history of cardiovascular risk factors is supportive of microvascular ischemia or vertebrobasilar insufficiency, though the presence of cardiovascular risk factors does not exclude other important causes discussed here.4,6
Localization and Suggested Imaging and Workup
Findings that suggest a cortical or brain stem lesion include altered mental status, weakness or numbness in the extremities, ataxia, vertigo, and/or bilateral cranial nerve deficits. MRI of the brain with and without gadolinium should be obtained.
Bilateral cranial nerve deficits can also occur due to pathology in the subarachnoid space such as infectious or carcinomatous meningitis. In addition to neuroimaging, select patients may require lumbar puncture.
In contrast, multiple unilateral cranial nerve deficits suggest a brain stem, cavernous sinus (CNs III, IV, V1, V2, VI), or orbit (CNs III, IV, V1, VI) lesion. Cavernous sinus and orbit lesions may also cause proptosis. MRI with and without gadolinium of the orbit is the preferred imaging modality for orbital lesions. CT or magnetic resonance (MR) venography is helpful for diagnosing cavernous sinus thrombosis, whereas CT or MR angiography is helpful for diagnosing a carotid-cavernous fistula.
All patients with isolated CN III palsy should undergo urgent MR or CT angiography of the brain to assess for intracranial aneurysm. Several studies have demonstrated that the presence of vascular risk factors and/or physical exam findings such as pupil involvement do not reliably distinguish between subacute causes such as microvascular ischemia and serious acute neurological disease.3,4,6
Most, if not all, patients with isolated CN IV or VI palsy should also undergo an urgent MRI of the brain with and without gadolinium. Historically, urgent neuroimaging was deferred in selected patients with isolated CN IV or VI palsy lacking high-risk features. However, this practice has been called into question by recent studies that have shown a significant proportion of patients have structural lesions evident on MRI that dictate changes in early management.4
Conclusion
Knowing the differential diagnosis and how to distinguish among the diverse causes of diplopia should enhance your confidence in your ability to assess important emergency neurological conditions. A thorough history and exam as well as appropriate neuroimaging and diagnostic testing can clinch the diagnosis, thereby saving a patient’s sight and maybe even their life.
Dr. Strong is a clinical instructor in the department of emergency medicine at Brigham and Women’s Hospital in Boston.
References
- Nazerian P, Vanni S, Tarocchi C, et al. Causes of diplopia in the emergency department: diagnostic accuracy of clinical assessment and of head computed tomography. Eur J Emerg Med. 2014;21(2):118-124.
- Tan A, Faridah H. The two-minute approach to monocular diplopia. Malays Fam Physician. 2010;5(3):115-118.
- Fang C, Leavitt JA, Hodge DO, et al. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol. 2017;135(1):23-28.
- Tamhankar MA, Biousse V, Ying GS, et al. Isolated third, fourth, and sixth cranial nerve palsies from presumed microvascular versus other causes: a prospective study. Ophthalmology. 2013;120(11):2264-2269.
- Ross AG, Jivraj I, Rodriguez G, et al. Retrospective, multicenter comparison of the clinical presentation of patients presenting with diplopia from giant cell arteritis vs other causes. J Neuroophthalmol. 2019;39(1):8-13.
- Chou KL, Galetta SL, Liu GT, et al. Acute ocular motor mononeuropathies: prospective study of the roles of neuroimaging and clinical assessment. J Neurol Sci. 2004;219(1-2):35-39.
The post How to Evaluate Diplopia and Spot Life-Threatening Etiologies appeared first on ACEP Now.